La SCSM proactive a-t-elle encore un rôle à jouer dans les MII : examen de la documentation
Résumé
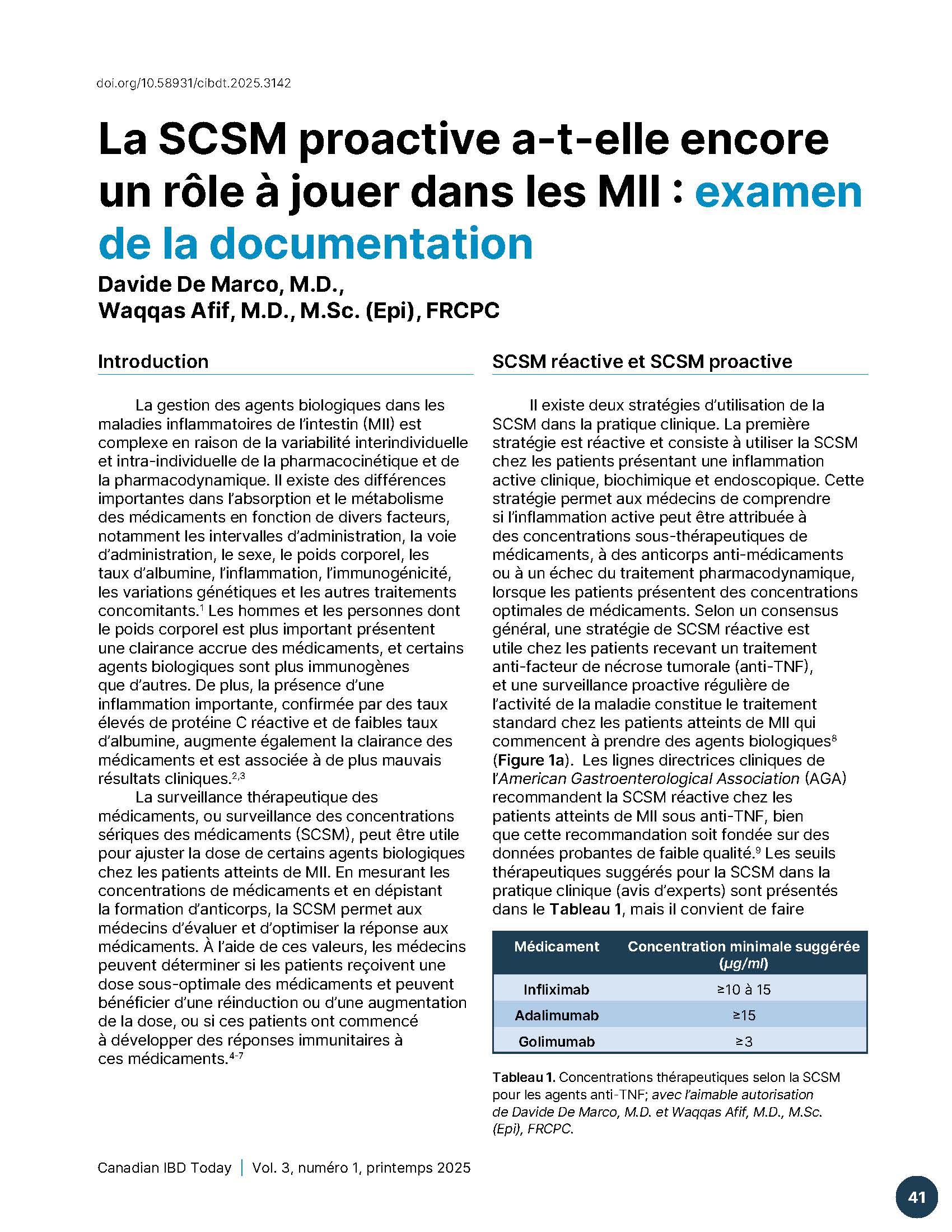
La gestion des agents biologiques dans les maladies inflammatoires de l’intestin (MII) est complexe en raison de la variabilité interindividuelle et intra-individuelle de la pharmacocinétique et de la pharmacodynamique. Il existe des différences importantes dans l’absorption et le métabolisme des médicaments en fonction de divers facteurs, notamment les intervalles d’administration, la voie d’administration, le sexe, le poids corporel, les taux d’albumine, l’inflammation, l’immunogénicité, les variations génétiques et les autres traitements concomitants. Les hommes et les personnes dont le poids corporel est plus important présentent une clairance accrue des médicaments, et certains agents biologiques sont plus immunogènes que d’autres. De plus, la présence d’une inflammation importante, confirmée par des taux élevés de protéine C réactive et de faibles taux d’albumine, augmente également la clairance des médicaments et est associée à de plus mauvais résultats cliniques.
La surveillance thérapeutique des médicaments, ou surveillance des concentrations sériques des médicaments (SCSM), peut être utile pour ajuster la dose de certains agents biologiques chez les patients atteints de MII. En mesurant les concentrations de médicaments et en dépistant la formation d’anticorps, la SCSM permet aux médecins d’évaluer et d’optimiser la réponse aux médicaments. À l’aide de ces valeurs, les médecins peuvent déterminer si les patients reçoivent une dose sous-optimale des médicaments et peuvent bénéficier d’une réinduction ou d’une augmentation de la dose, ou si ces patients ont commencé à développer des réponses immunitaires à ces médicaments.
Références
Lefevre PL, Shackelton LM, Vande Casteele N. Factors influencing drug disposition of monoclonal antibodies in inflammatory bowel disease: implications for personalized medicine. BioDrugs. 2019;33(5):453-68.
Fasanmade AA, Adedokun OJ, Ford J, Hernandez D, Johanns J, Hu C, et al. Population pharmacokinetic analysis of infliximab in patients with ulcerative colitis. European journal of clinical pharmacology. 2009;65:1211-28.
Ordás I, Mould DR, Feagan BG, Sandborn WJ. Anti‐TNF monoclonal antibodies in inflammatory bowel disease: pharmacokinetics‐based dosing paradigms. Clinical Pharmacology & Therapeutics. 2012;91(4):635-46.
Kennedy NA, Heap GA, Green HD, Hamilton B, Bewshea C, Walker GJ, et al. Predictors of anti-TNF treatment failure in anti-TNF-naive patients with active luminal Crohn’s disease: a prospective, multicentre, cohort study. The lancet Gastroenterology & hepatology. 2019;4(5):341-53.
Papamichael K, Cheifetz AS, Melmed GY, Irving PM, Casteele NV, Kozuch PL, et al. Appropriate therapeutic drug monitoring of biologic agents for patients with inflammatory bowel diseases. Clinical Gastroenterology and Hepatology. 2019;17(9):1655-68. e3.
Shukla R, Ananthakrishnan A. Therapeutic drug monitoring of non-anti-tumor necrosis factor biologics. Clinical Gastroenterology and Hepatology. 2021;19(6):1108-10.
Papamichael K, Afif W, Drobne D, Dubinsky MC, Ferrante M, Irving PM, et al. Therapeutic drug monitoring of biologics in inflammatory bowel disease: unmet needs and future perspectives. The lancet Gastroenterology & hepatology. 2022;7(2):171-85.
Colombel J-F, Panaccione R, Bossuyt P, Lukas M, Baert F, Vaňásek T, et al. Effect of tight control management on Crohn’s disease (CALM): a multicentre, randomised, controlled phase 3 trial. The Lancet. 2017;390(10114):2779-89.
Feuerstein JD, Nguyen GC, Kupfer SS, Falck-Ytter Y, Singh S, Gerson L, et al. American Gastroenterological Association Institute guideline on therapeutic drug monitoring in inflammatory bowel disease. Gastroenterology. 2017;153(3):827-34.
Singh S, Dulai PS, Vande Casteele N, Battat R, Fumery M, Boland BS, et al. Systematic review with meta‐analysis: association between vedolizumab trough concentration and clinical outcomes in patients with inflammatory bowel diseases. Alimentary pharmacology & therapeutics. 2019;50(8):848-57.
Casteele NV, Herfarth H, Katz J, Falck-Ytter Y, Singh S. American Gastroenterological Association Institute technical review on the role of therapeutic drug monitoring in the management of inflammatory bowel diseases. Gastroenterology. 2017;153(3):835-57. e6.
Meserve J, Ma C, Dulai PS, Jairath V, Singh S. Effectiveness of reinduction and/or dose escalation of ustekinumab in Crohn’s disease: a systematic review and meta-analysis. Clinical Gastroenterology and Hepatology. 2022;20(12):2728-40. e1.
Peyrin-Biroulet L, Danese S, Argollo M, Pouillon L, Peppas S, Gonzalez-Lorenzo M, et al. Loss of response to vedolizumab and ability of dose intensification to restore response in patients with Crohn’s disease or ulcerative colitis: a systematic review and meta-analysis. Clinical Gastroenterology and Hepatology. 2019;17(5):838-46. e2.
Sandborn WJ, Su C, Sands BE, D’Haens GR, Vermeire S, Schreiber S, et al. Tofacitinib as induction and maintenance therapy for ulcerative colitis. New England Journal of Medicine. 2017;376(18):1723-36.
Sandborn WJ, Peyrin-Biroulet L, Sharara AI, Su C, Modesto I, Mundayat R, et al. Efficacy and safety of tofacitinib in ulcerative colitis based on prior tumor necrosis factor inhibitor failure status. Clinical Gastroenterology and Hepatology. 2022;20(3):591-601. e8.
Muensterman E, Engelhardt B, Gopalakrishnan S, Anderson JK, Mohamed MEF. Upadacitinib pharmacokinetics and exposure‐response analyses of efficacy and safety in psoriatic arthritis patients–Analyses of phase III clinical trials. Clinical and Translational Science. 2022;15(1):267-78.
Ponce-Bobadilla AV, Stodtmann S, Eckert D, Zhou W, Liu W, Mohamed M-EF. Upadacitinib population pharmacokinetics and exposure-response relationships in ulcerative colitis patients. Clinical Pharmacokinetics. 2023;62(1):101-12.
Danese S, Vermeire S, Zhou W, Pangan AL, Siffledeen J, Greenbloom S, et al. Upadacitinib as induction and maintenance therapy for moderately to severely active ulcerative colitis: results from three phase 3, multicentre, double-blind, randomised trials. The lancet. 2022;399(10341):2113-28.
Loftus Jr EV, Panés J, Lacerda AP, Peyrin-Biroulet L, D’Haens G, Panaccione R, et al. Upadacitinib induction and maintenance therapy for Crohn’s disease. New England Journal of Medicine. 2023;388(21):1966-80.
Sandborn WJ, Feagan BG, D’Haens G, Wolf DC, Jovanovic I, Hanauer SB, et al. Ozanimod as induction and maintenance therapy for ulcerative colitis. New England Journal of Medicine. 2021;385(14):1280-91.
Sands BE, Schreiber S, Blumenstein I, Chiorean MV, Ungaro RC, Rubin DT. Clinician’s guide to using ozanimod for the treatment of ulcerative colitis. Journal of Crohn’s and Colitis. 2023;17(12):2012-25.
Sethi S, Dias S, Kumar A, Blackwell J, Brookes MJ, Segal JP. Meta‐analysis: The efficacy of therapeutic drug monitoring of anti‐TNF‐therapy in inflammatory bowel disease. Alimentary Pharmacology & Therapeutics. 2023;57(12):1362-74.
Nguyen NH, Solitano V, Vuyyuru SK, MacDonald JK, Syversen SW, Jørgensen KK, et al. Proactive therapeutic drug monitoring versus conventional management for inflammatory bowel diseases: a systematic review and meta-analysis. Gastroenterology. 2022;163(4):937-49. e2.
Peyrin–Biroulet L, Deltenre P, De Suray N, Branche J, Sandborn WJ, Colombel JF. Efficacy and safety of tumor necrosis factor antagonists in Crohn’s disease: meta-analysis of placebo-controlled trials. Clinical Gastroenterology and Hepatology. 2008;6(6):644-53.
Lv R, Qiao W, Wu Z, Wang Y, Dai S, Liu Q, et al. Tumor necrosis factor alpha blocking agents as treatment for ulcerative colitis intolerant or refractory to conventional medical therapy: a meta-analysis. PloS one. 2014;9(1):e86692.
Hanauer SB, Feagan BG, Lichtenstein GR, Mayer LF, Schreiber S, Colombel JF, et al. Maintenance infliximab for Crohn’s disease: the ACCENT I randomised trial. The Lancet. 2002;359(9317):1541-9.
Hanauer SB, Sandborn WJ, Rutgeerts P, Fedorak RN, Lukas M, MacIntosh D, et al. Human anti–tumor necrosis factor monoclonal antibody (adalimumab) in Crohn’s disease: the CLASSIC-I Trial. Gastroenterology. 2006;130(2):323-33.
Colombel JF, Sandborn WJ, Rutgeerts P, Enns R, Hanauer SB, Panaccione R, et al. Adalimumab for maintenance of clinical response and remission in patients with Crohn’s disease: the CHARM trial. Gastroenterology. 2007;132(1):52-65.
Reinisch W, Sandborn WJ, Rutgeerts P, Feagan BG, Rachmilewitz D, Hanauer SB, et al. Long-term infliximab maintenance therapy for ulcerative colitis: the ACT-1 and-2 extension studies. Inflammatory bowel diseases. 2012;18(2):201-11.
Colombel JF, Sandborn WJ, Reinisch W, Mantzaris GJ, Kornbluth A, Rachmilewitz D, et al. Infliximab, azathioprine, or combination therapy for Crohn’s disease. New England journal of medicine. 2010;362(15):1383-95.
Seow CH, Newman A, Irwin SP, Steinhart AH, Silverberg MS, Greenberg GR. Trough serum infliximab: a predictive factor of clinical outcome for infliximab treatment in acute ulcerative colitis. Gut. 2010;59(01):49-54.
Maser EA, Villela R, Silverberg MS, Greenberg GR. Association of trough serum infliximab to clinical outcome after scheduled maintenance treatment for Crohn’s disease. Clinical Gastroenterology and Hepatology. 2006;4(10):1248-54.
Adedokun OJ, Sandborn WJ, Feagan BG, Rutgeerts P, Xu Z, Marano CW, et al. Association between serum concentration of infliximab and efficacy in adult patients with ulcerative colitis. Gastroenterology. 2014;147(6):1296-307. e5.
Cornillie F, Hanauer SB, Diamond RH, Wang J, Tang KL, Xu Z, et al. Postinduction serum infliximab trough level and decrease of C-reactive protein level are associated with durable sustained response to infliximab: a retrospective analysis of the ACCENT I trial. Gut. 2014;63(11):1721-7.
Papamichael K, Gils A, Rutgeerts P, Levesque BG, Vermeire S, Sandborn WJ, et al. Role for therapeutic drug monitoring during induction therapy with TNF antagonists in IBD: evolution in the definition and management of primary nonresponse. Inflammatory bowel diseases. 2015;21(1):182-97.
Vande Casteele N, Papamichael K, Jeyarajah J, Osterman M, Cheifetz A. DOP45 Adequate infliximab exposure during the induction phase is associated with early complete fistula response in patients with fistulizing Crohn’s disease: a post-hoc analysis of the ACCENT-2 trial. Journal of Crohn’s and Colitis. 2019;13(Supplement_1):S053-S4.
Battat R, Lukin D, Scherl EJ, Pola S, Kumar A, Okada L, et al. Immunogenicity of tumor necrosis factor antagonists and effect of dose escalation on anti-drug antibodies and serum drug concentrations in inflammatory bowel disease. Inflammatory bowel diseases. 2021;27(9):1443-51.
Casteele NV, Ferrante M, Van Assche G, Ballet V, Compernolle G, Van Steen K, et al. Trough concentrations of infliximab guide dosing for patients with inflammatory bowel disease. Gastroenterology. 2015;148(7):1320-9. e3.
D’Haens G, Vermeire S, Lambrecht G, Baert F, Bossuyt P, Pariente B, et al. Increasing infliximab dose based on symptoms, biomarkers, and serum drug concentrations does not increase clinical, endoscopic, and corticosteroid-free remission in patients with active luminal Crohn’s disease. Gastroenterology. 2018;154(5):1343-51. e1.
Assa A, Matar M, Turner D, Broide E, Weiss B, Ledder O, et al. Proactive monitoring of adalimumab trough concentration associated with increased clinical remission in children with Crohn’s disease compared with reactive monitoring. Gastroenterology. 2019;157(4):985-96. e2.
Seow CH, Marshall JK, Stewart E, Pettengell C, Ward R, Afif W. The relationship among vedolizumab drug concentrations, biomarkers of inflammation, and clinical outcomes in a Canadian real-world study. Journal of the Canadian Association of Gastroenterology. 2024;7(4):290-8.
Porth R, Deyhim T, Zullow S, Rabinowitz LG, Grossberg LB, Roblin X, et al. Proactive therapeutic drug monitoring is associated with increased drug persistence in patients with inflammatory bowel disease treated with intravenous vedolizumab. Inflammatory Bowel Diseases. 2024:izae140.
Jairath V, Yarur A, Osterman MT, James A, Balma D, Mehrotra S, et al. ENTERPRET: a randomized controlled trial of vedolizumab dose optimization in patients with ulcerative colitis who have early nonresponse. Clinical Gastroenterology and Hepatology. 2024;22(5):1077-86. e13.
Porth R, Deyhim T, Geeganage G, Smith B, Zullow S, Rabinowitz LG, et al. Proactive Therapeutic Drug Monitoring of Ustekinumab Is Associated With Increased Drug Persistence in Patients With Inflammatory Bowel Disease. Inflammatory Bowel Diseases. 2024:izae231.
Wang Z, Hoffert Y, Zhang W, Kantasiripitak W, Verstockt B, Sabino J, et al. OP12 Therapeutic antibody clearance better predicts endoscopic outcomes than trough concentrations in patients with Crohn’s disease. Journal of Crohn’s and Colitis. 2025;19(Supplement_1):i24-i6.
Wu J-F. Therapeutic drug monitoring of biologics for patients with inflammatory bowel diseases: how, when, and for whom? Gut and Liver. 2021;16(4):515.
Publié
Comment citer
Numéro
Rubrique
Licence
© Canadian IBD Today 2025

Cette œuvre est sous licence Creative Commons Attribution - Pas d'Utilisation Commerciale - Pas de Modification 4.0 International.